General
- intellectual disability
- opioid withdraw
- central line complications
- testicular cancer
- alternative medicine
- palliative care
- rapid sequence intubation
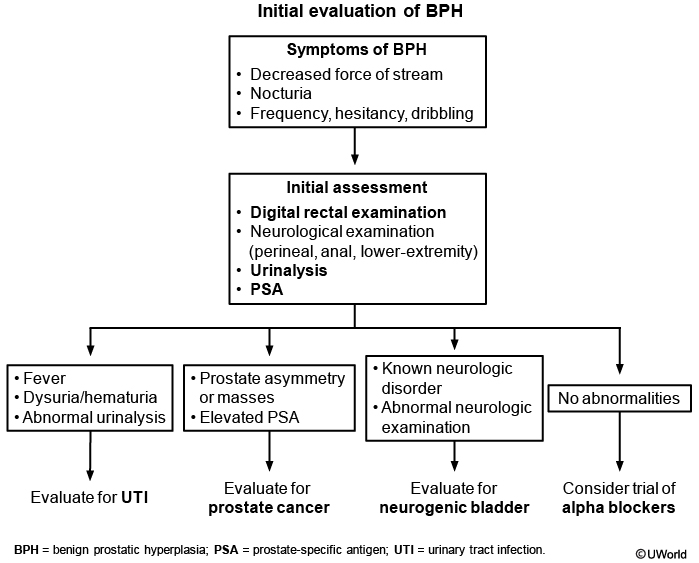
- BPH
- code status
- airway management
- goals of care
- capacity and competency
- medicare medicaid
- blood draw
- SSRI side effects
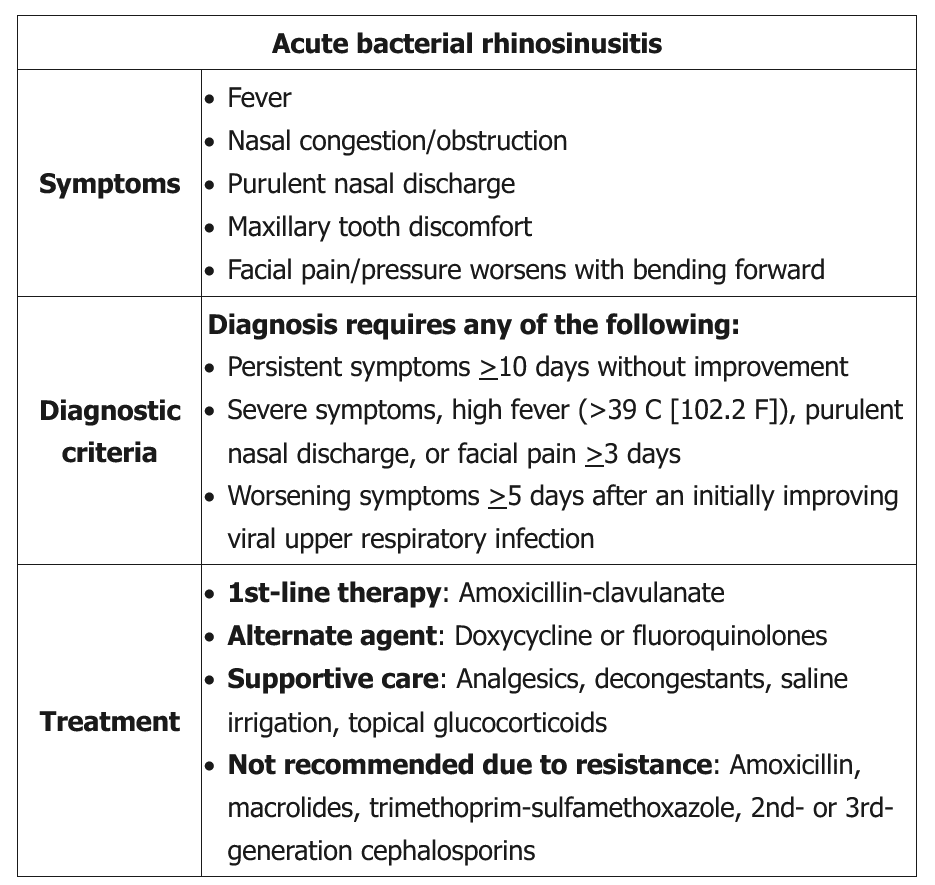
- acute bacterial sinusitis
- tobacco smoking cessation
- dry mouth can be treated with cevimeline or other muscarinics
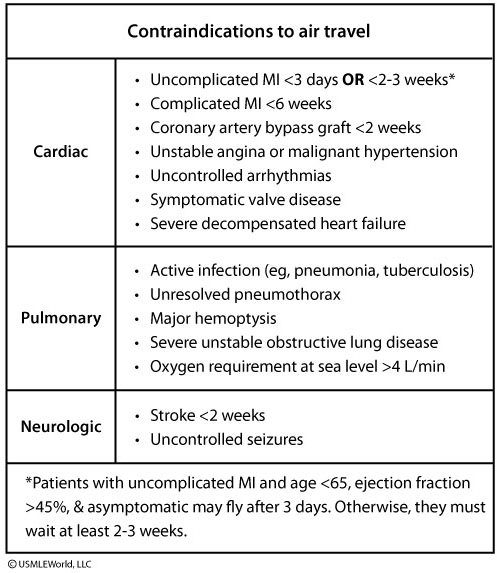
- contraindications to air travel
- managing frostbite
- ACE I with amlodipine leads to less peripheral edema
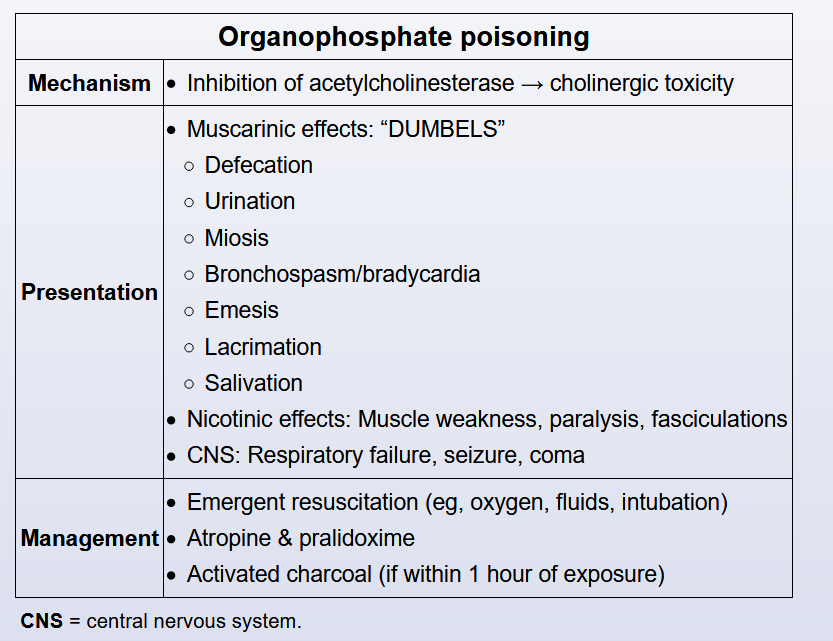
Poisoning
Poison
Arsenic's first-line chelating agent is dimercaprol (eg, British Anti-Lewisite), which increases urinary excretion of heavy metals by forming stable, nontoxic soluble chelates.
Acute lead poisoning can present with constipation, anemia, and irritability and confusion. CaNa2EDTA is a treatment option for lead toxicity and works by forming non-ionizing salts to increase urinary lead excretion.
Deferoxamine is the preferred chelating agent for iron overdoses or overload due to multiple blood transfusions. It binds circulating iron and facilitates its urinary excretion.
Stress Ulcers
1 factor:
- Coagulopathy: platelets <50,000/mm3, INR >1.5, PTT >2x normal control
- Mechanical ventilation >48 hours
- GI bleeding or ulceration in last 12 months
- Head trauma, spinal cord injury, major burn
2 factors:
- Glucocorticoid therapy
- >1 week ICU stay
- Occult GI bleeding >6 days
- Sepsis
This mechanically ventilated patient with recent head trauma has developed an upper gastrointestinal (GI) bleed, as evidenced by the melenic bowel movements and anemia. This is most likely from gastric or esophageal stress ulcers. Critically ill patients may have uremic toxins and reflux of bile salts into the stomach; both can disrupt the protective glycoprotein layer, which can lead to increased permeability of the gastric mucosa, predisposing to ulcer formation. Head trauma causes increased gastrin secretion, leading to parietal cell stimulation and acid secretion. Shock is associated with mucosal ischemia leading to ulcerations. Most of these ulcerations occur within the first 72 hours and tend to be located in the proximal stomach. Ulcerations occurring later in the hospital course tend to be located in the duodenum.
Proton pump inhibitors (PPIs) as well as H2 antagonists are used to increase the pH in the stomach by lowering gastric acid formation, which prevents the gastric injury associated with ulcer formation. PPI may have increased efficacy in acid suppression. Both PPIs and H2 antagonists may be associated with increased risk of Clostridium difficile infection (CDI) and pneumonia.
Kidney donations
- Inability to consent (age <18, intellectual disability, untreated psychiatric disease)
- Diabetes mellitus
- Hypertension with end-organ dysfunction
- BMI >35 kg/m2
- Malignancy
The most important factors in matching a kidney donor to a recipient include human leukocyte antigen (HLA) matching and ABO compatibility. In addition, kidney transplants from living donors, when available, have better outcomes than those from deceased donors. Compared with deceased kidney donation, living donated kidneys have longer graft survival. Finally, transplant outcomes are best when the transplant can be performed before the patient requires dialysis (pre-emptive transplantation). Because living donor organs are available sooner, the need for dialysis can be limited or avoided entirely. Size is generally not a consideration, as transplanted kidneys are placed in a different location from the native kidneys.
TURP
Retrograde ejaculation is the most frequent complication of transurethral resection of the prostate (TURP), which is an invasive procedure used in the management of benign prostatic hyperplasia (BPH).
Urinary tract infections and urethral strictures are also complications of TURP, but are less common.
Urinary incontinence and erectile dysfunction have been described with TURP but are relatively uncommon.
Flex Sig
Flexible sigmoidoscopy requires less preparation and is an acceptable alternative. If findings are normal, it should be repeated at 5-year intervals (or 10-year intervals if combined with annual fecal immunochemical testing).
However, sigmoidoscopy does not visualize the proximal colon and is less sensitive than colonoscopy. Increased risk for advanced neoplasia in the proximal colon is seen with:
- Large (>1.0 cm) adenomatous polyps
- Multiple adenomatous polyps
- Polyps with villous or tubulovillous morphology
Therefore, all patients who have such polyps detected on sigmoidoscopy should have visualization of the entire colon with colonoscopy.
Tetanus
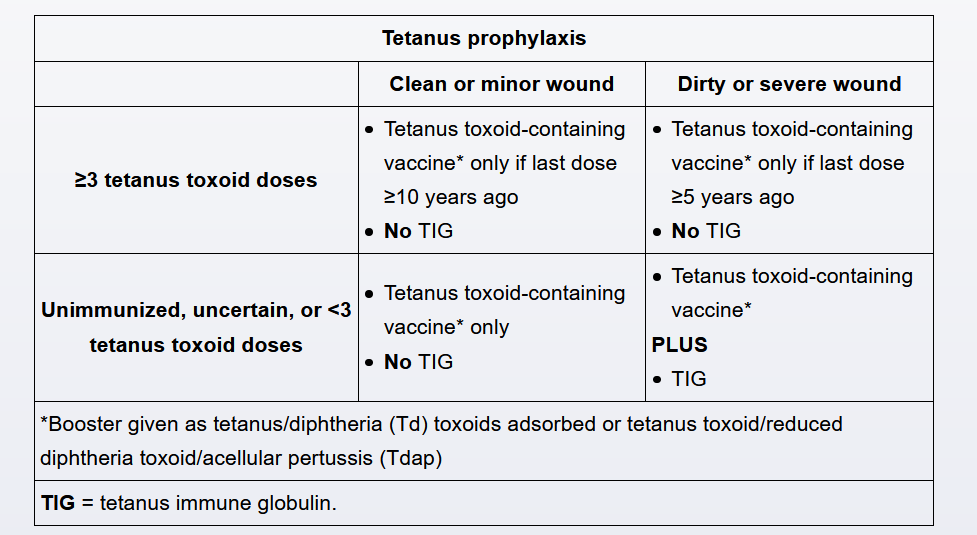
Following a mammalian bite, the decision to administer tetanus prophylaxis (ie, tetanus toxoid-containing vaccine ± tetanus immune globulin) is based on the severity of the wound and the immunization status of the patient.
- For patients who have received ≥3 tetanus toxoid doses, a booster dose of tetanus toxoid is indicated only if their last tetanus dose was ≥10 years ago (for clean or minor wounds) or ≥5 years ago (for dirty or severe wounds).
- Patients who have received <3 tetanus toxoid doses (ie, incompletely immunized) or whose vaccine status is uncertain should receive a tetanus toxoid booster. If such patients have dirty or severe wounds, they should also receive tetanus immune globulin.
This child has severe wounds with evidence of contamination (eg, bite wound, specks of dirt, plant matter). However, the child is up to date on immunizations, which means he has received at least 4 tetanus toxoid-containing vaccines (ie, diphtheria, tetanus toxoid, and acellular pertussis [DTaP] at age 2, 4, and 6 months and an additional DTaP at 4 years). His last dose was <5 years ago. Therefore, there is no need for either a tetanus toxoid booster or tetanus immune globulin
Pneumococcal
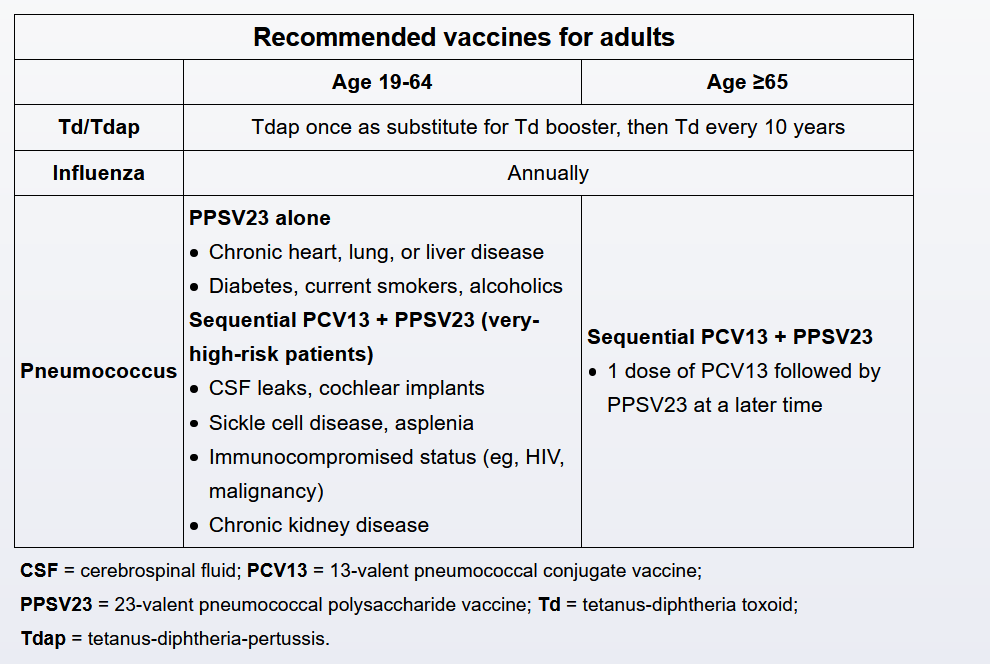
The 13-valent conjugated pneumococcal vaccine (PCV13) is recommended for all adults age >65; it should be followed by the 23-valent pneumococcal polysaccharide vaccine (PPSV23) 6-12 months later (Choice B). Sequential PCV13 and PPSV23 are also recommended for adults age <65 with certain high risk underlying conditions (eg, cerebrospinal fluid [CSF] leaks, sickle cell disease, cochlear implants, congenital/acquired asplenia, immunocompromise, chronic renal failure). PPSV23 alone is recommended for adults age <65 with other chronic medical conditions including smoking, diabetes, heart or lung disease, and chronic liver disease.
Coin ingestion
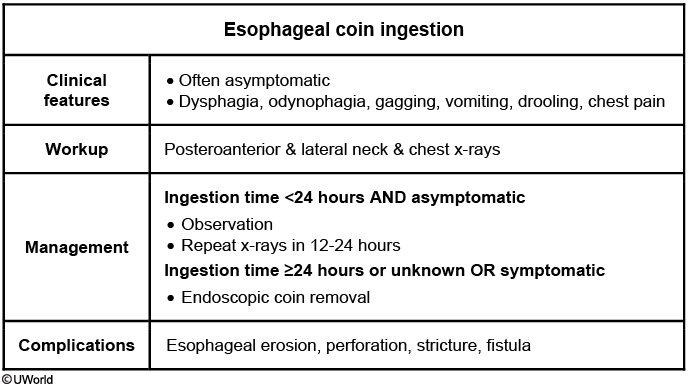
Foreign body ingestion is common in toddlers, and coins are the most commonly swallowed objects. Management depends on symptoms, time of ingestion, and the type of object ingested. Children are not reliable historians and many events are unwitnessed. A 2-view (posteroanterior [PA] and lateral) neck and chest x-ray confirms the location of the foreign body and distinguishes between a coin and battery (the latter can cause perforation in just a few hours). A coin is seen in this patient's x-ray as a homogenous object with a sharp, crisp edge; the bilaminar structure of a button battery causes a "double-ring" sign.
Children who swallow coins are often asymptomatic, but some have dysphagia and drooling. Asymptomatic patients with coin ingestion <24 hours earlier can be observed with repeat x-rays in 12-24 hours to ensure passage beyond the pylorus (Choice C). Children who had an unknown time of ingestion, such as this patient, or those who are symptomatic should undergo flexible endoscopy for coin removal. Coins lodged >24 hours are at significant risk for complications (eg, erosion, perforation).
Emergency bronchoscopy would be appropriate for an airway foreign body causing respiratory compromise. This patient has no stridor, wheezing, or respiratory distress and the lateral radiograph indicates that the foreign body is in the esophagus rather than the airway. In addition, an esophageal coin appears linear on lateral x-ray; a tracheal coin appears linear (project on end) in the PA view.
Gout HTN
This patient has uncontrolled hypertension that has failed lifestyle interventions. Hypertension must be managed cautiously in patients with gout. Most diuretics (eg, hydrochlorothiazide, furosemide) decrease the fractional excretion of urate and should be avoided when possible (Choice E). This patient's serum uric acid level is at goal, but an increase could put him at risk for further gout flares.
The angiotensin II receptor blocker losartan has a mild uricosuric effect and is effective as first-line treatment for hypertension in patients with gout. If additional lowering of blood pressure is needed, calcium channel blockers (eg, amlodipine) are safe to use in gout and work well in combination with angiotensin II receptor blockers.
(Choice B) Beta blockers with alpha-blocking activity (eg, labetalol, carvedilol) are not recommended as first-line treatment for hypertension. Beta blockers are generally associated with an increased risk of gout flare.
Varicocele
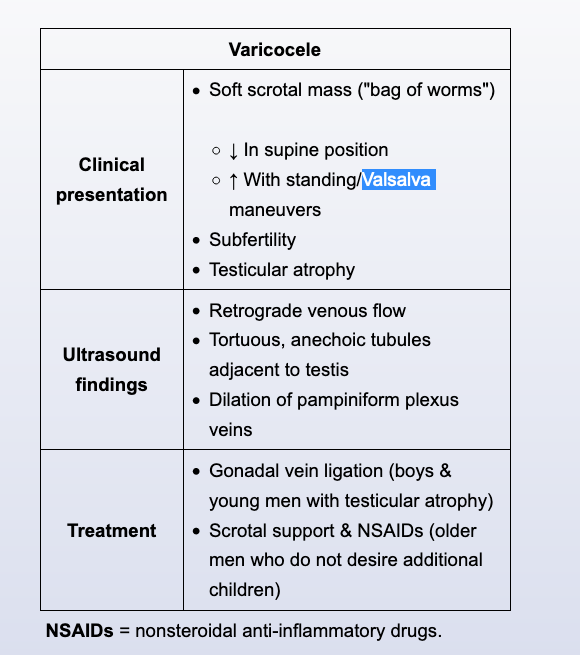
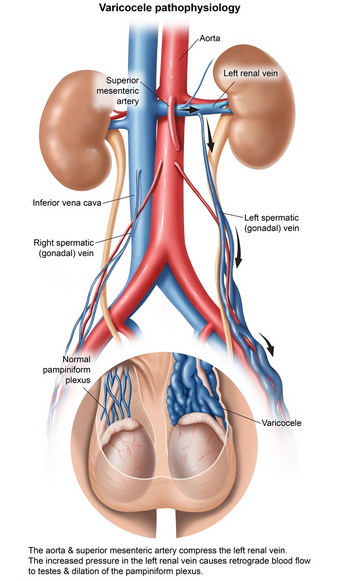
A varicocele is a tortuous dilation of veins in the pampiniform plexus surrounding the spermatic cord and testis. It occurs in nearly 20% of postpubertal males and presents as a soft, irregular mass ("bag of worms") that increases in size with standing and Valsalva. Varicoceles can cause elevated scrotal temperatures, increasing the risk for infertility and testicular atrophy. Patients with varicoceles do not have an increased risk of testicular cancer.
If needed, the diagnosis can be confirmed by ultrasound, which can show retrograde venous flow and dilation of pampiniform plexus. Asymptomatic patients do not require treatment. Those with scrotal discomfort usually improve with analgesics (eg, nonsteroidal anti-inflammatory drugs) and/or scrotal support. Patients with testicular atrophy or infertility may benefit from surgery to improve fertility.
The left spermatic vein drains to the left renal vein, which then passes between the superior mesenteric artery and the aorta. Compression beneath the superior mesenteric artery ("nutcracker effect") can lead to increased pressure in the spermatic vein and venous dilation. For this reason, varicoceles are more common on the left side. In contrast, the right spermatic vein drains directly into the inferior vena cava, and right-sided varicoceles are relatively rare. A right-sided varicocele can be a sign of malignant compression (eg, renal cell carcinoma) and therefore warrants CT imaging. CT scan is not recommended for workup of an isolated, left-sided varicocele.
Acetaminophen toxicity
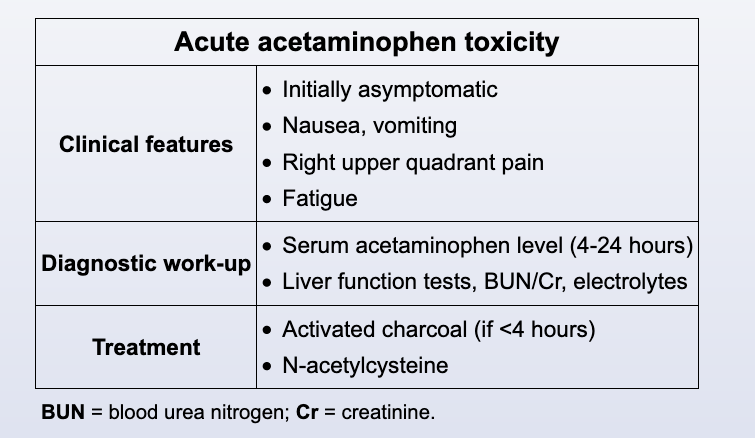
Acetaminophen poisoning can occur from an acute intentional ingestion of a toxic dose (150 mg/kg in children, 7.5 g in adults). Following ingestion, patients typically go through 4 clinical stages: nonspecific symptoms or asymptomatic (0-24 hours), hepatotoxicity (24-72 hours), peak of liver function abnormalities (72-96 hours), and recovery (4-14 days).
Patients who present within 4 hours of ingestion are given activated charcoal for gastric decontamination (Choice A). Acetaminophen level is then obtained at 4 hours post-ingestion, and the level is correlated with the time since ingestion on the Rumack-Matthew nomogram to determine whether the antidote, N-acetylcysteine (NAC), is required. Levels are not measured <4 hours after ingestion because they are unreliable and poor predictors of toxicity.
If presentation is 4-24 hours after ingestion, as in this patient, acetaminophen concentration is measured immediately, and empiric NAC is administered while awaiting the results. Prompt administration of NAC is recommended, even in asymptomatic patients, ideally before the onset of liver injury, as this antidote is highly effective in preventing hepatotoxicity. Aspartate transaminase, alanine transaminase, blood urea nitrogen, and creatinine are measured to assess for hepatic injury and hepatorenal syndrome. If the acetaminophen level remains above the treatment line on the nomogram, NAC is continued.
Liver failure is rare in children and adolescents who receive NAC early. Although those with fulminant hepatic failure and hepatic encephalopathy may require liver transplantation, this patient is currently asymptomatic and should first receive NAC.
Except in rare cases, gastric lavage is not recommended for gastric decontamination due to the significant risk for aspiration pneumonia.
GBS
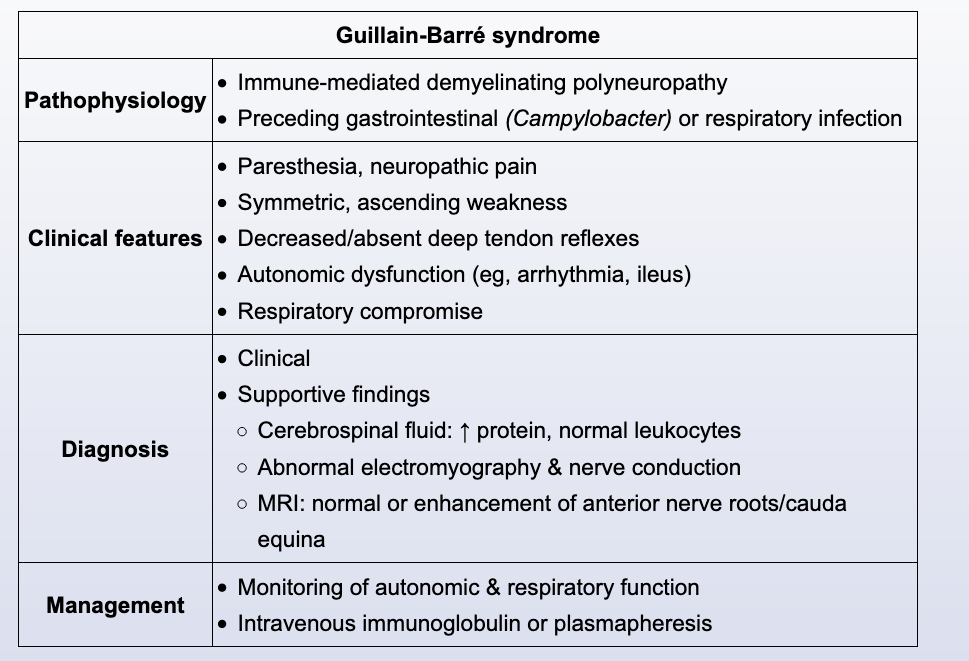
This patient with paresthesias, autonomic dysfunction, shortness of breath, and symmetric motor weakness likely has Guillain-Barré syndrome (GBS).
GBS is an acute, immune-mediated polyneuropathy due to cross-reacting antibodies against peripheral nerve components. Most cases are preceded by a gastrointestinal (eg, Campylobacter) or respiratory infection. Major manifestations include:
- Progressive symmetric motor weakness (usually beginning in the legs)
- Hyporeflexia
- Paresthesias
- Autonomic dysfunction (eg, palpations, orthostatic hypotension)
- Respiratory, facial, and/or oropharyngeal muscle weakness
The diagnosis of GBS is largely clinical, but suspicion is supported by characteristic cerebrospinal fluid (high protein with normal leukocytes) and electrodiagnostic studies. Treatment with intravenous immunoglobulin or plasmapheresis can shorten time to recovery. Most patients recover completely but some have residual neurologic sequelae.
DAN
This patient most likely has overflow urinary incontinence (OUI) due to diabetic autonomic neuropathy (DAN). In patients with longstanding diabetes mellitus, microvascular damage often leads to neuropathy affecting the autonomic nervous system. Autonomic parasympathetic innervation controls contraction of the detrusor muscle during urination; impaired detrusor muscle contraction due to DAN or other autonomic nerve injury (eg, spinal cord trauma, multiple sclerosis) leads to urinary retention, elevated intravesicular pressure, and eventually OUI. This patient's orthostatic hypotension provides additional evidence of autonomic impairment due to DAN.
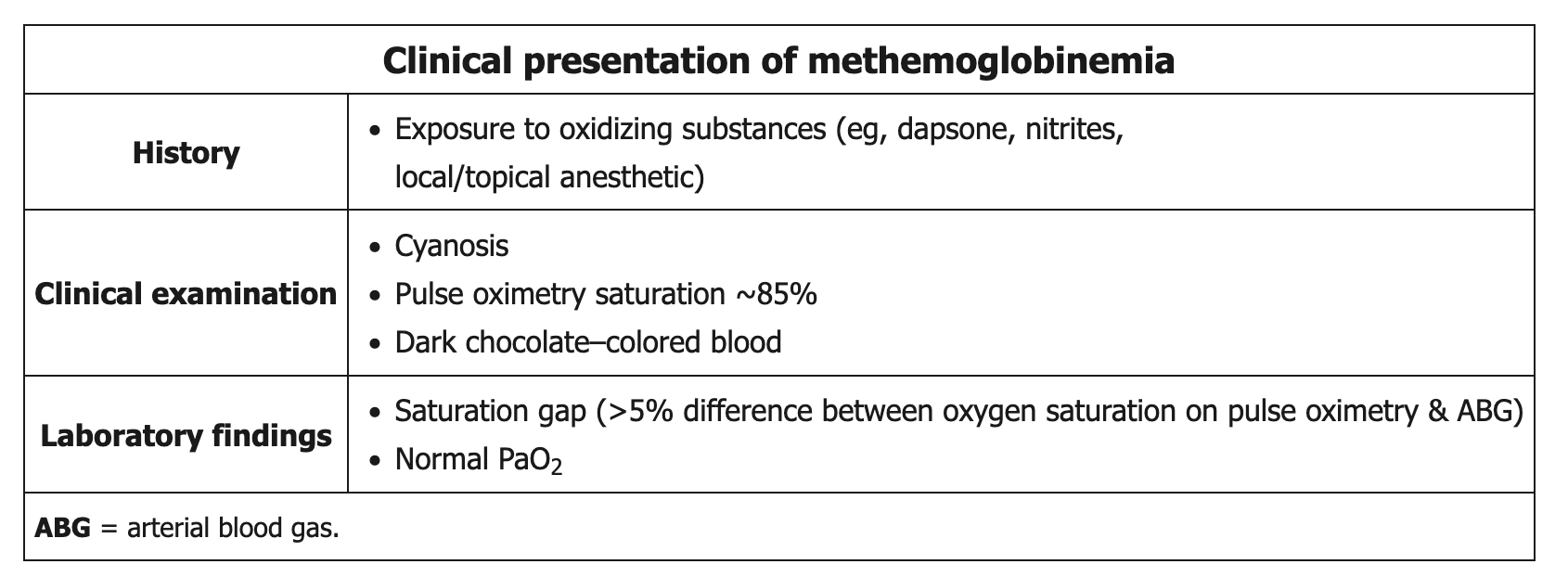 Methemoglobinemia is most commonly acquired after excessive exposure to an oxidizing agent (eg, dapsone, nitrites, local/topical anesthetics such as benzocaine/lidocaine (surgical patients)). Methemoglobin is a form of hemoglobin in whi
Methemoglobinemia is most commonly acquired after excessive exposure to an oxidizing agent (eg, dapsone, nitrites, local/topical anesthetics such as benzocaine/lidocaine (surgical patients)). Methemoglobin is a form of hemoglobin in whi