Anemia
Microcytic anemia
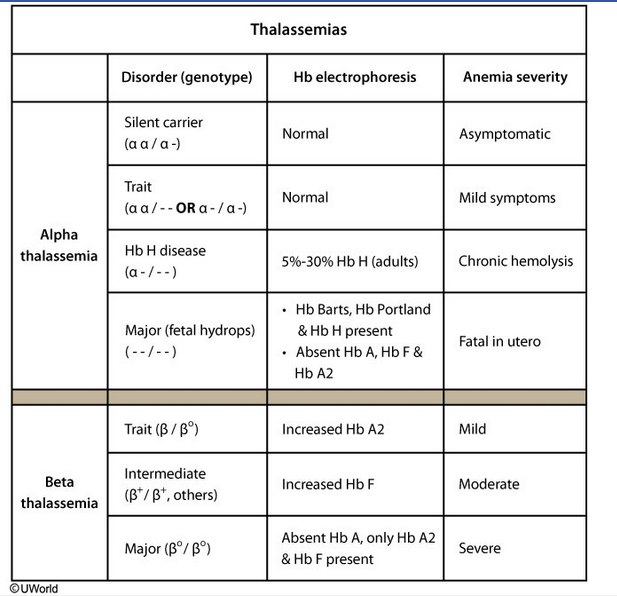
Thalassemia
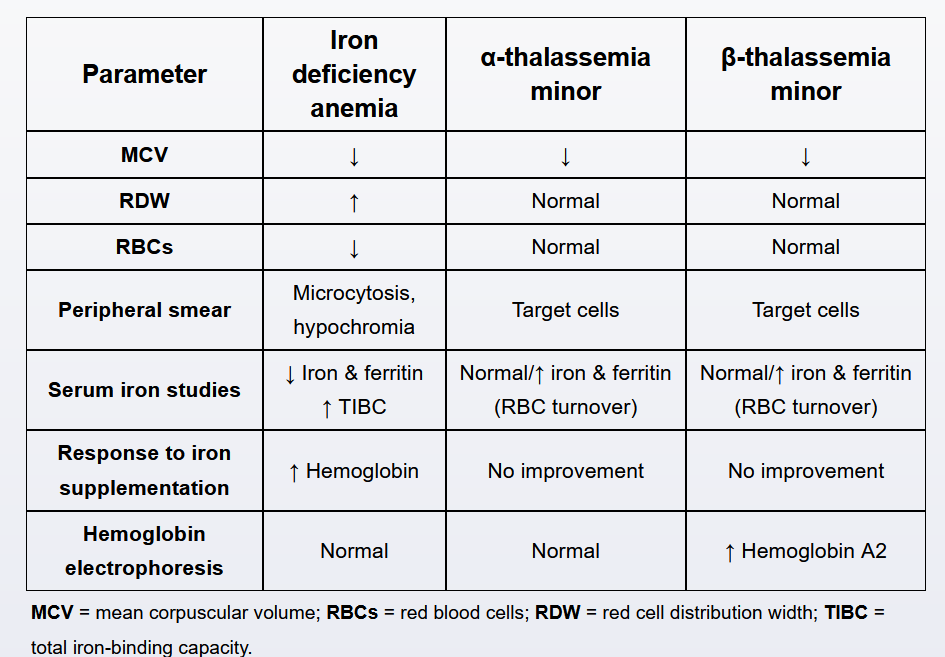
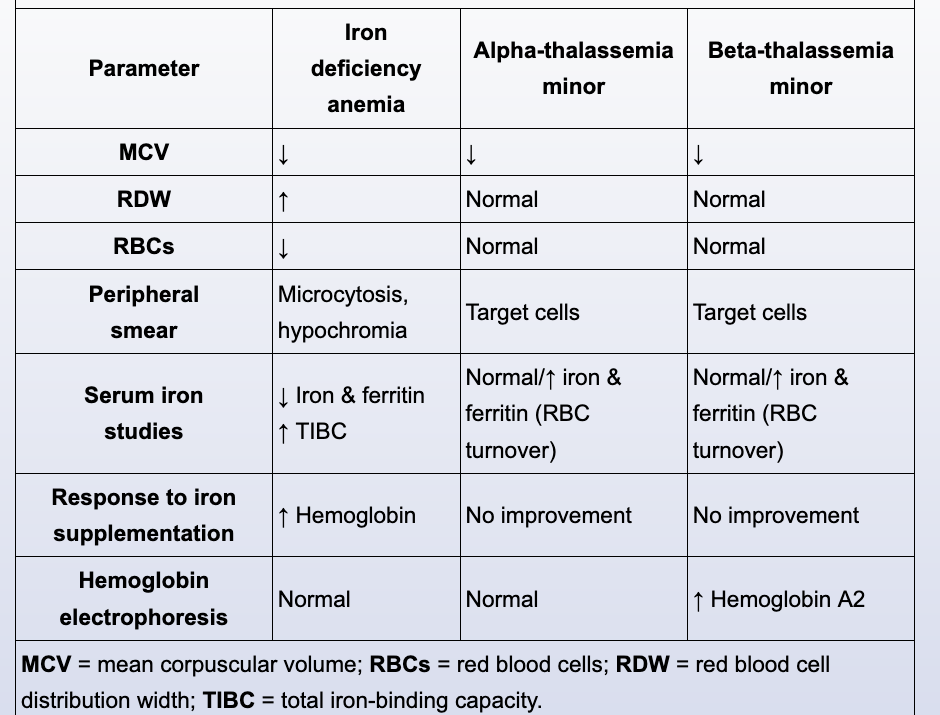
Screening for anemia is routine at the first prenatal visit. Patients with thalassemia minor (ie, thalassemia trait) have mild microcytic, hypochromic anemia, as indicated by a low mean corpuscular volume (MCV) and mean corpuscular hemoglobin, respectively. They also have mildly elevated ferritin due to increased red blood cell (RBC) turnover. The RBC count may be normal or increased, but the red cell distribution width (RDW) is normal as almost all RBCs are uniformly small. In addition, the anemia is relatively mild in comparison with the decrease in MCV.
This patient's results are consistent with thalassemia minor, which is common in those of Mediterranean, Middle Eastern, Southeast Asian, African, and Indian descent. A maternal hemoglobin electrophoresis should be ordered to confirm the diagnosis and distinguish α- from β-thalassemia minor. Electrophoresis is normal in patients with α-thalassemia; β-thalassemia causes abnormally elevated hemoglobin A2 levels.
After confirmation of maternal thalassemia, a paternal hemoglobin electrophoresis is indicated to determine the fetal risk of thalassemia major. Maternal conditions requiring partner testing include clinically significant maternal hemoglobinopathies (eg, SS, SC, hemoglobin S/β-thalassemia) as well as carrier states (α- and β-thalassemia minor).
Thalaseemia