Amenorrhea
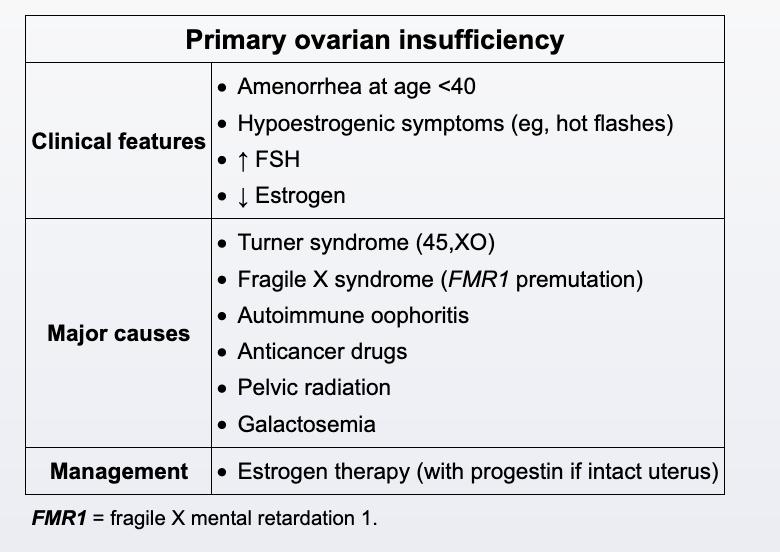
This patient has amenorrhea with low estrogen, elevated FSH, and hypoestrogenic symptoms. This is consistent with primary ovarian insufficiency (POI), which is a common complication of cancer treatment with chemotherapy and radiation therapy. In addition, she has low bone density as evidenced by a low (age-adjusted) Z-score on DXA. Patients with POI can rapidly lose bone mass, leading to an increased risk of fragility fractures.
In the absence of specific risk factors (eg, history of breast cancer), most patients with POI should receive oral or transdermal estrogen therapy, which should be combined with a progestin in women with an intact uterus to reduce the risk of endometrial cancer. Estrogen therapy can relieve hypoestrogenic symptoms (eg, hot flashes, vaginal dryness) and minimize bone loss. Estrogen replacement should be continued until the average age of normal menopause, around age 50. Postmenopausal estrogen/progesterone therapy is associated with significant risks (eg, venous thromboembolism, coronary heart disease), but the absolute risks are substantially lower in young patients with POI, and the benefits far outweigh the risks for most patients.
Functional amenorrhea
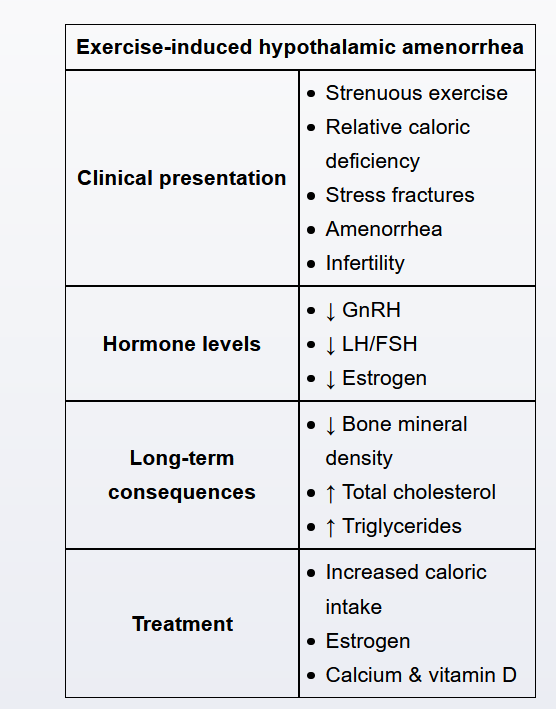
Patients with functional hypothalamic amenorrhea (FHA) typically have amenorrhea, a low BMI, and findings of estrogen deficiency (breast atrophy). Additional features include anovulatory infertility and vaginal atrophy with dyspareunia. Female athletes are particularly susceptible to FHA due to a relative caloric deficiency associated with strenuous physical activity and high energy expenditure; other causes include stress and anorexia nervosa. The relative caloric deficiency results in decreased levels of GnRH resulting in decreased LH and FSH levels, suppressed ovarian function, and low estrogen levels.
Patients with FHA also have an increased risk of bone fracture due to increased bone resorption from inadequate caloric intake. Therefore, a bone mineral density measurement (eg, DXA) is indicated in these patients. This constellation of symptoms (eg, oligomenorrhea or amenorrhea, relative caloric deficiency, decreased bone mineral density) constitutes the athlete triad that characterizes FHA. Treatment includes increased caloric intake, calcium and vitamin D supplementation, and estrogen for bone loss prevention.
However, she also has amenorrhea; exogenous GH use is not associated with menstrual irregularities. In addition, patients using exogenous GH typically have associated hypertension and fluid retention (eg, edema, carpal tunnel syndrome), which are not seen in this patient.